
From the 1Department of Neurology, Neurorehabilitation Unit, Vivantes Klinikum Spandau, 2Neurology at Wittenbergplatz, Berlin, 3Department of Neurology, Asklepios Klinik Barmbek, Hamburg and 4Fresenius Academy, Idstein, Germany
Objective: Clinical parameters for prediction of post-stroke spasticity are well established. This report introduces 2 brain magnetic resonance imaging (MRI) parameters (infarct volume and topographic distribution) as post-stroke spasticity predictors.
Methods: Topographic and volumetric data from brain MRI for 98 patients with ischaemic stroke with spasticity, prevalent within the first 5 days after stroke and 6 months after stroke, were retrospectively correlated using Chris Rorden’s MRIcron software.
Results: Lesions within the supply territory of the middle cerebral artery involving the pyramidal tract were more frequently associated with spasticity than without spasticity (30.8% vs 5.1%). Middle cerebral artery lesions not affecting the pyramidal tract were found more often in patients without spasticity (49.2% vs 10.3%). Spasticity showed a significantly higher association with middle cerebral artery+pyramidal tract/internal capsule lesions than did “no spasticity” (97.5% vs 18.7%, p < 0.01), and lesion volumes were significantly larger in patients with spasticity than in those without spasticity (p < 0.01).
Conclusion: Large stroke volumes might predict post-stroke spasticity if the lesion is > 3 cm3 in size and if the lesion is located within the middle cerebral artery territory with involvement of the pyramidal tract and/or internal capsule. Lesion size ≤ 2 cm3 outside the middle cerebral artery territory is associated with lower risk of post-stroke spasticity.
Key words: stroke; spasticity; magnetic resonance imaging; prediction.
Accepted Mar 3, 2020; Epub ahead of print Mar 12, 2020
J Rehabil Med 2020; 52: jrm00065
Correspondence address: Anatol Kivi, Department of Neurology, Neurorehabilitation Unit, Vivantes Klinikum Spandau, Berlin, Germany. E-mail: anatol.kivi@vivantes.de
Clinical parameters for the prediction of post-stroke spasticity (PSS) are well established. We report here 2 parameters from brain magnetic resonance imaging (MRI) (infarct volume and topographic distribution) as predictors of PSS. Topographic and volumetric brain MRI data from 98 patients with ischaemic stroke were studied retrospectively and correlated with the prevalence of spasticity (within 5 days after stroke) using Chris Rorden’s MRIcron software. Lesions within the supply territory of the middle cerebral artery involving the pyramidal tract and/or internal capsule were significantly more frequently associated with spasticity than without spasticity. Middle cerebral artery lesions not affecting the pyramidal tract were found more frequently in patients without spasticity. Lesions in the middle cerebral artery territory with pyramidal tract/internal capsule involvement had a significantly higher association with spasticity than with “no spasticity”. Lesion volumes were larger in patients with spasticity than in those without spasticity. Large stroke volumes can predict PSS if ≥3 cm3 and if located in the middle cerebral artery territory with involvement of the pyramidal tract and/or internal capsule.
Spastic movement disorder (SMD) is a common sequela of stroke and is one of the positive signs of upper motor neurone syndrome (UMNS). In addition to the patient’s individual disabilities and discomfort in daily living the therapeutic challenge for rehabilitation, as well as the large-scale socio-economic impact of SMD after stroke (post-stroke spasticity; PSS), is undisputed and tremendous (1–5).
Attempts have been made to predict PSS by use of several parameters, particularly clinical assessments. For instance, Urban et al. denoted upper limb muscle tone increase and impairment of sensorimotor function as the most important clinical predictors for PSS (6). Over and above a pure clinical evaluation, data from brain magnetic resonance imaging (MRI) appears to be highly promising for prediction of PSS with respect to anatomical and aetiological considerations (7–10).
The mechanisms for developing spasticity after stroke are far from fully understood. However, an alteration in the modulating influence of descending fibre tracts on spinal local networks is widely accepted as one of the most relevant pathophysiological changes. Such descending fibre tracts include the pyramidal tract, in which cortical neurones mainly target bulbar and spinal interneurones via the hind limb of the capsula interna, pons, and lateral and anterior corticospinal tract. Other descending systems of the motor system include the reticulospinal and rubrospinal tract, which are also known to be recruited for patient’s dexterity after pyramidal tract lesions (11). Despite the obviously pivotal role of these descending motor systems, from our experience, we know that not all ischaemic brain lesions lead to PSS. The aim of this retrospective study is, therefore, to evaluate both the volume and distribution of ischaemic brain lesions as MRI predictors for PSS. We test the hypothesis that there are lesions in distinct regions of the brain and of distinct volume size (cut-off) that are capable of positive or negative prediction of PSS, respectively.
Study design
Retrospective conditional comparative study.
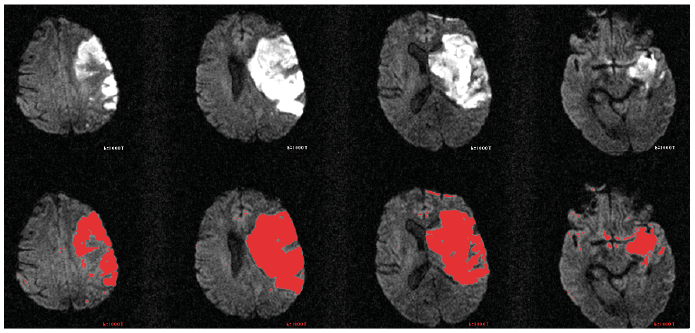
From a cohort of 301 consecutive patients with stroke (aged between 17 and 96 years) with UMNS due to a first-ever ischaemic stroke, 211 patients were clinically examined at baseline (within 5 days after stroke) as well as 6 months later (for demographic data, see Urban et al. (6)). The data collected by Urban et al. (6) includes a brain MRI data-set in most cases in addition to the anamnestic and clinical data. From this data-set only predictors of clinical PSS were published (6). The clinical assessment was carried out using the modified Ashworth scale (MAS). Spasticity was classified as present if MAS was ≥ 1 for any passive movement. Of 211 patients, 98 were eligible for retrospective analysis of topographic and volumetric data from brain MRI of ischaemic brain lesions (5 days after stroke, Chris Rorden’s MRIcron software (Chris Rorden, McCausland Center for Brain Imaging, Columbia, South Carolina, USA); Fig. 1). All other 113 patients were lost due to lack of MRI, death, recurrent stroke, or due to reassessment being declined by the patient (6). Thirty-seven patients of 98 (37.8%) were female. Topographic patterns and lesion volumes were compared between patients with and without spasticity, using Mann–Whitney U test and χ2 test. Statistical analysis was performed using SPSS 21.0.
Fig. 1. Example of an acute ischaemic stroke in the territory of the right middle cerebral artery in 4 diffusion-weighted horizontal magnetic resonance (MR) images (DWI, upper line). Voxel counting of the lesion and volume calculation are based on manually selected lesion regions in each MR slice (red, bottom line).
Demographic data for all 98 patients included in the study are shown in Table I. Of these, 39 patients (39.8%) had PSS (MAS ≥ 1) in at least one limb, whereas 59 (60.2%) showed no spasticity within the baseline period of the first 5 days after stroke or 6 months later.
Lesion site
The following lesion sites were associated with PSS and selected for further analysis (12–15): (i) middle cerebral artery territory (MCA) including the pyramidal tract; (ii) MCA territory not including the pyramidal tract; (iii) anterior cerebral artery territory (ACA) or ACA/MCA; (iv) posterior cerebral artery territory (PCA) or MCA/PCA; (v) basal ganglia; (vi) thalamus; (vii) posterior limb of the internal capsule (IC) (anterior choroidal artery, AChA); (viii) brainstem; and (ix) cerebellum (Table II).
A lesion within the MCA territory involving the pyramidal tract (MCA-PT), or a lesion affecting the posterior limb of the IC appeared significantly more frequently in patients with spasticity than in patients without spasticity (MCA-PT 30.8% vs 5.1%; IC 66.7% vs 13.6%; Fig. 2). Conversely, MCA lesions sparing the pyramidal tract were found significantly more often in patients without spasticity (49.2% vs 10.3%). There was no correlation of “spasticity” vs “no spasticity” with respect to MRI lesions in all brain regions other than MCA involving PT (MCAPT) or IC (Table II). MCAPT and IC, and all other regions (“non-MCA/PT/IC”) were grouped together, respectively. Thus, lesions were found in MCAPT and/or IC in 38 out of 39 patients (97.5%) in patients with PSS, compared with only 11 out of 59 (18.7%) without spasticity (Table II).
Table I. Demographics of participants (n = 98)
Table II. Lesion location in patients with and without spasticity (n = 98)
Lesion size
Overall, significantly larger brain lesion volumes were found in patients with spasticity than in those without spasticity (a mean of 44.28 cm3 in the spasticity group (median 4.76 cm3; Q1–Q3 2.63–38.1 cm3) vs 20.65 cm3 (median 2.04; Q1–Q3 1.07–11.65 cm3) in the non-spasticity group, respectively (p < 0.01; Mann-Whitney U test)). Despite this, a relatively large proportion of patients without spasticity showed large lesion volumes of > 10 cm3 (14 of 59 non-spastic patients = 23.7%). Next, this study attempted to narrow down the lesion volumes to transition points with relevant changes in PSS. Almost logarithmically grouped volumes (0.1, 0.2, 0.3, 0.5, 1, 2, 3, 5, 7, 8, 10, 20, 30, 50, 70, 80, 100 cm3, larger) were analysed for correlation of lesion volume and PSS. The 18 volume group sizes were not significantly different between the spasticity group and the non-spasticity group (p > 0.05). In general, only flat volume peaks were found (< 25% each; Fig. 3, Table III). Out of these peaks the highest volume peaks, found at 2 and 5 cm3 (n = 18 (18.4%) and n = 16 (16.3%), respectively) as well as one volume in between (3 cm3), were chosen for cut-off-value analysis. Lower peaks were found at 1, 3, 20 and 100 cm3 (Table III). To test for possible volume cut-off values to enable a positive or negative PSS prediction in the MCAPT/IC group and non-MCAPT/IC group, respectively, the sensitivity (positive prediction) and specificity (negative prediction) were calculated for the volume-peaks 2, 3 and 5 cm3. It was found that a combination of a small infarct volume (≤ 2 cm3) without MCAPT/IC affection was the strongest negative predictor for PSS (negative predictive value (NPV): 95.8%, odds ratio (OR): 61.33, Table IV). By contrast, if a lesion volume >3 cm3 involved the MCAPT /IC the positive predictive value (PPV) of PSS was 76.7% (OR 28.48). Further increase in the lesion volume ≥ 5 cm3 did not proportionally enhance the prediction values compared with the other cut-off values (PPV 72.7% and NPV 869.7%, OR 17.07).
Fig. 2. Frequency of affected MC+APT/IC in patients with (orange) and without (blue) spasticity, respectively. MCAPT: middle cerebral artery territory involving pyramidal tract; IC: internal capsule.
Fig. 3. Sorting of ischaemic brain lesions with respect to lesion volume in patients with affected (orange, n = 44) and not affected (blue, n = 54) middle cerebral artery involving pyramidal tract (MC+APT) and/or internal capsule, respectively.
Table III. Distribution of lesions volumes in 98 patients with and without affected middle cerebral artery involving pyramidal tract (MCAPT) and/or internal capsule (IC), respectively
Table IV. Sensitivity and specificity of lesion volumes and locations in prediction of post-stroke spasticity (PSS)
These data show that both volume and location of ischaemic brain lesions, especially large-sized lesions including the PT and/or the IC, can predict the development of PSS. Small lesion volumes, ≤2 cm3, which do not affect the PT/IC are of negative predictive value for development of PSS within 6 months after stroke. Large lesion volumes, >3 cm3, affecting the pyramidal tract are of positive predictive value for the development of PSS.
Underlining the findings of Urban et al. (6) regarding pure clinical PSS-predictors, the MRI data from the same patient cohort shows that calculating lesion volume and infarct location might be an additional and promising tool for prediction of PSS. The data from the current study reinforce and expand the results of other groups dealing with brain imaging as PSS predictor, in that MRI lesion volume and distribution might be a valuable early predictor of PSS (12–15). However, our post-hoc analysis did not allow us to judge the relevance of imaging vs not-imaging PSS-predictors, which should be reassessed in a sufficiently powered prospective study. Finally, the current study was methodologically incap-able of tracking PSS-relevant affected sub-components of the pyramidal and parapyramidal systems in detail, which might be done by use of MR-based fibre tracking. However, our data may be used as the basis for future studies focussing on minimum volumes and bounded localizations of ischaemic brain lesions.
This study was supported by Allergan GmbH, Frankfurt am Main, Germany. Data analysis, writing, review & editing, visualizations, supervision, and project administration was made independently by the authors.


 Click to show fullsize
Click to show fullsize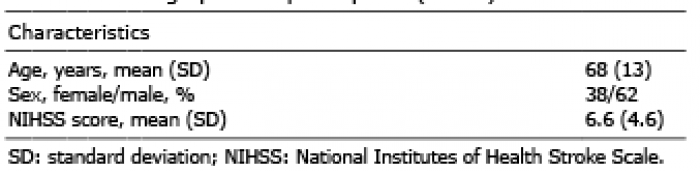 Click to show fullsize
Click to show fullsize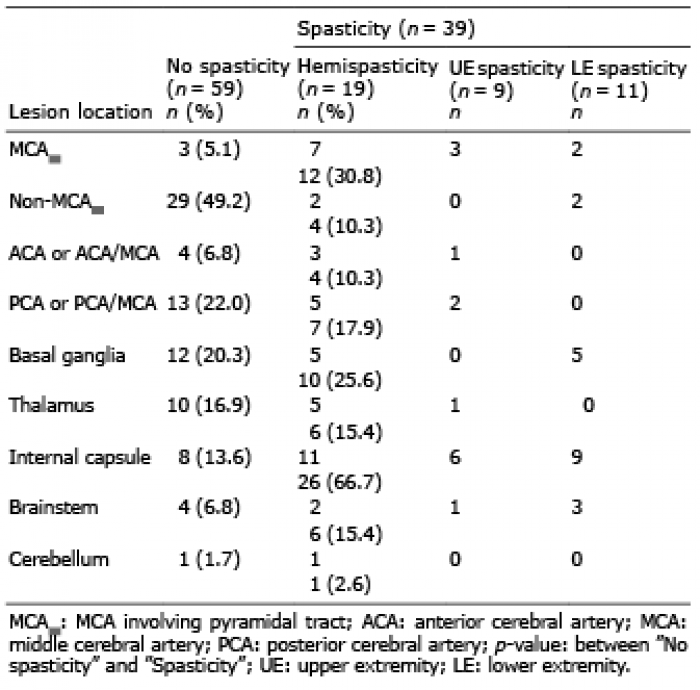 Click to show fullsize
Click to show fullsize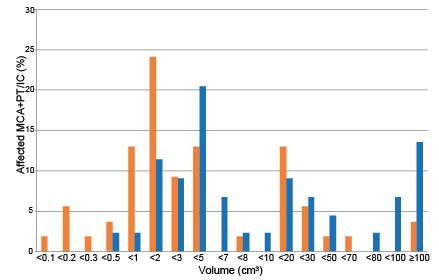 Click to show fullsize
Click to show fullsize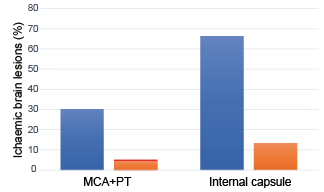 Click to show fullsize
Click to show fullsize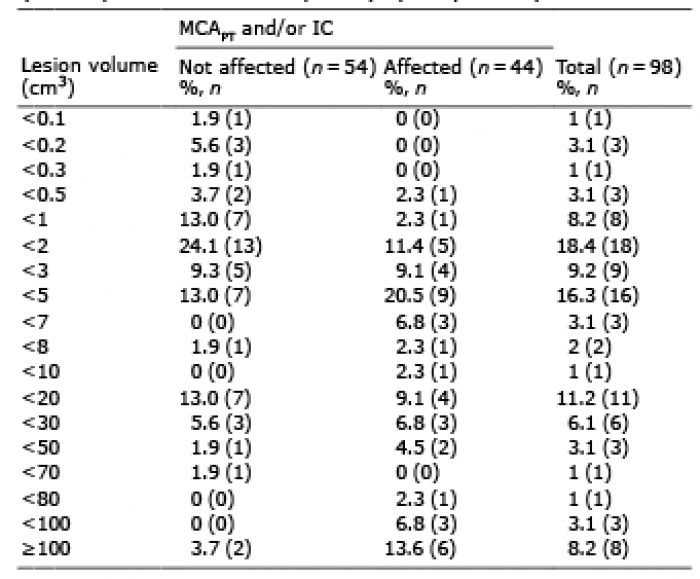 Click to show fullsize
Click to show fullsize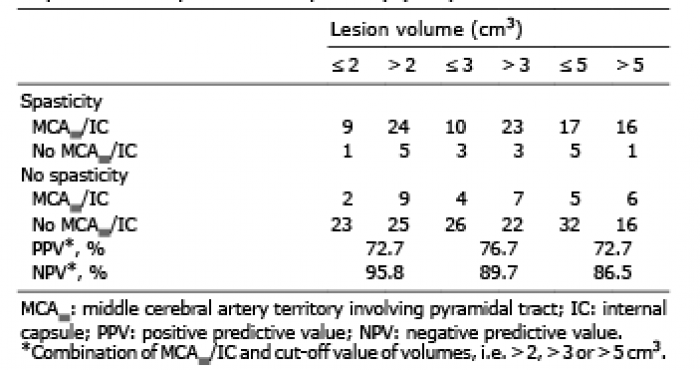 Click to show fullsize
Click to show fullsize